 |
Case Report
Distal femur fractures, when double plate is mandatory: A case report
1 MD, Department of Orthopaedics, Centro Hospitalar de Leiria, 2410-197 Leiria, Portugal
Address correspondence to:
Nuno José Abrantes Botelho Mai
Rua de Santo André, 2401-197 Leiria,
Portugal
Message to Corresponding Author
Article ID: 100022O03NM2024
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Maia NJAB, Marto É, Rodrigues F, Oliveira F, Silva JD, Caetano JP. Distal femur fractures, when double plate is mandatory: A case report. Edorium J Orthop 2024;9(1):5–8.ABSTRACT
Introduction: Distal femoral fractures pose significant challenges in terms of surgical management due to their complex anatomy and potential for non-union.
Case Report: This article presents a case study of a 44-year-old male patient who sustained an open comminuted distal femur fracture following a road accident, highlighting the treatment approach and outcomes. Definitive treatment involved the use of both lateral and medial distal femoral plates, employing a double approach.
Conclusion: The discussion emphasizes the importance of addressing factors such as medial metaphyseal comminution and osteoporosis in achieving stable fixation and reducing the risk of failure. The utilization of double plates is advocated as a mean to stabilize both distal femoral columns, thereby enhancing stability and promoting successful outcomes in challenging fractures.
Keywords: Distal femur fracture, Double approach, Medial plate, Trauma
INTRODUCTION
Distal femoral fractures represent 3–6% of femoral fractures, accounting for 0.4% of all fractures [1]. They present a bimodal distribution. Despite the reduced prevalence, osteosynthesis can be complex, requiring anatomical reduction and sufficiently stable fixation to allow early mobility of the knee [2]. Historically, osteosynthesis is based on the use of locked lateral plates and is associated with a non-union rate that can reach up to 20% [2],[3].
CASE REPORT
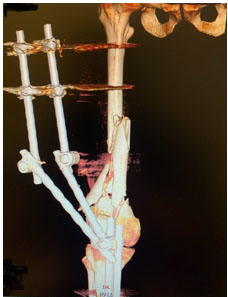
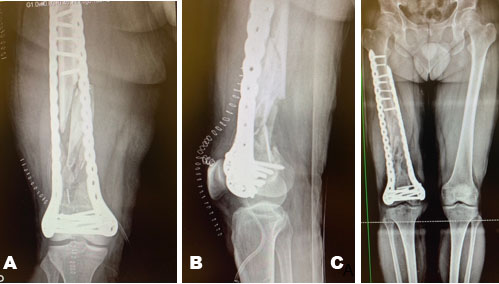
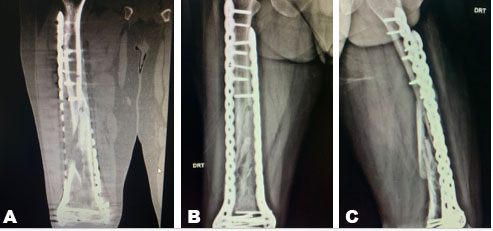
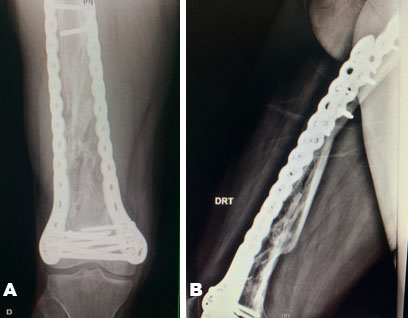
We present the case of a 44-year-old male patient who suffered a Gustillo-Anderson Grade IIIA exposed distal femur fracture (classification AO33C3) after a road accident (Figure 1). Initially he underwent cleaning and debridement and osteotaxis with external fixators (Figure 2). At two weeks definitive treatment was carried out using lateral distal femoral and medial femoral plates, with a double approach—lateral and medial (Figure 3). Due to the comminution of the fracture, full exposure of the fracture site was needed for correct reconstruction, with the plates acting as bridging plates. The patient had an uneventful postoperative period. At six months postoperatively he had limited mobility (0–50° of flexion) and radiological examinations showed delay on the consolidation of the fracture site (Figure 4). He underwent new surgery—quadricepsplasty, decortication, and application of an autograft. After this new intervention, he progressed well clinically with follow-up at 12 months with complete mobility and consolidation of the fracture on radiological examinations (Figure 5).

DISCUSSION
Medial metaphyseal comminution, osteoporotic bone, and insufficient fixation lead to varus collapse or non-union in this type of fracture [4],[5]. The use of double plates allows the two distal columns of the femur (lateral and medial) to be stabilized, resulting in stable fixation in supracondylar comminuted femoral fractures, low periprosthetic fractures and in cases of non-union [6],[7],[8],[9],[10].
CONCLUSION
The adjuvant use of a medial plate reduces the rate of osteosynthesis failure while not resulting in an increase in intraoperative bleeding losses or surgical complications, with equal functional results.
REFERENCES
1.
Elsoe R, Ceccotti AA, Larsen P. Population-based epidemiology and incidence of distal femur fractures. Int Orthop 2018;42(1):191–6. [CrossRef]
[Pubmed]

2.
Hake ME, Davis ME, Perdue AM, Goulet JA. Modern implant options for the treatment of distal femur fractures. J Am Acad Orthop Surg 2019;27(19):e867–75. [CrossRef]
[Pubmed]
3.
Beltran MJ, Gary JL, Collinge CA. Management of distal femur fractures with modern plates and nails: State of the art. J Orthop Trauma 2015;29(4):165–72.
[Pubmed]
4.
Bolhofner BR, Carmen B, Clifford P. The results of open reduction and Internal fixation of distal femur fractures using a biologic (indirect) reduction technique. J Orthop Trauma 1996;10(6):372–7. [CrossRef]
[Pubmed]
5.
Davison BL. Varus collapse of comminuted distal femur fractures after open reduction and internal fixation with a lateral condylar buttress plate. Am J Orthop (Belle Mead NJ) 2003;32(1):27–30.
[Pubmed]
6.
Vallier HA, Hennessey TA, Sontich JK, Patterson BM. Failure of LCP condylar plate fixation in the distal part of the femur. A report of six cases. J Bone Joint Surg Am 2006;88(4):846–53. [CrossRef]
[Pubmed]
7.
Ricci WM, Streubel PN, Morshed S, Collinge CA, Nork SE, Gardner MJ. Risk factors for failure of locked plate fixation of distal femur fractures: An analysis of 335 cases. J Orthop Trauma 2014;28(2):83–9. [CrossRef]
[Pubmed]
8.
Park KH, Oh CW, Park IH, Kim JW, Lee JH, Kim HJ. Additional fixation of medial plate over the unstable lateral locked plating of distal femur fractures: A biomechanical study. Injury 2019;50(10):1593–8. [CrossRef]
[Pubmed]
9.
DeKeyser GJ, Hakim AJ, O’Neill DC, Schlickewei CW, Marchand LS, Haller JM. Biomechanical and anatomical considerations for dual plating of distal femur fractures: A systematic literature review. Arch Orthop Trauma Surg 2022;142(10):2597–609. [CrossRef]
[Pubmed]
10.
Tripathy SK, Mishra NP, Varghese P, et al. Dual-plating in distal femur fracture: A systematic review and limited meta-analysis. Indian J Orthop 2021;56(2):183–207. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Author Contributions
Nuno José Abrantes Botelho Mai - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Érica Marto - Drafting the work, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Francisco Rodrigues - Acquisition of data, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Fernando Oliveira - Acquisition of data, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
João Diogo Silva - Acquisition of data, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
João Pedro Caetano - Conception of the work, Design of the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guaranter of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2024 Nuno José Abrantes Botelho Maia et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.



